 |
|
RECOMMENDED CONCISE
|
|
Marketing Science and Misinformation
|
|
|
|
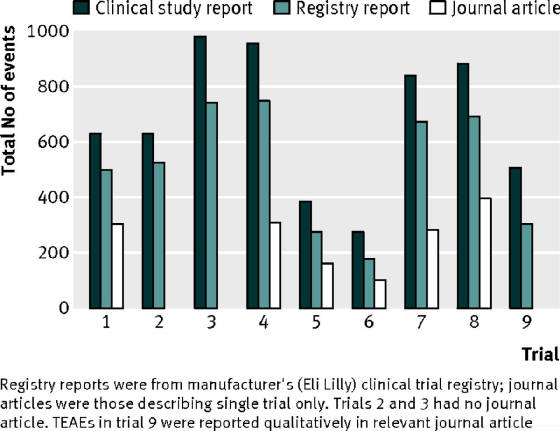
| raw data is clinical trial |
|
| journal articles hide side effect 65% of times |
The topic is central to
the making of
wise medical choices. It is central to
your accepting the well supported conclusions that are in the following
articles on this site which run counter to corporate medicine.. An understanding
of how bad things have
gotten is worth another essay. If you
need convincing please read the next article at http://healthfully.org/rc/id9.html. Highly recommended
is Junk treatments, which explains the methods pharma used to turn physicians into pill pushers. . As Dr. Philippe Even, the
author
of "The Guide to the 4,000 Useful,
Useless or Dangerous Medicines" told The Guardian: “The pharmaceutical
industry is the most lucrative, the most cynical and the least ethical of all
the industries. It is like an octopus with tentacles that has infiltrated all
the decision-making bodies: world health
organizations, government agencies, parliaments, high administrations in health
and hospitals and the medical profession." My 10 years of developing the
website http://healthfully.org has confirmed that
summation. You
should take better care of your health than your car.
at link are a collection of documentaries
confirm the claims made below about pharma and the state of medicine.
A few additions will be added, because of additional methods of pharma that I have uncovered
relying upon those professor who stood up (see http://healthfully.org/critics/ ) and others.
Marketing
Science and Misinformation—2pg—jk,
11/23/15 http://healthfully.org/rc/id1.html
All
the
issue raised below can be also found in “The
Truth About the Drug Companies,
by Marcia Angell, MD,
Harvard Professor, by David
Healy article, and book Pharmagaddon,
and those listed on my critics
page. This work conforms
to academic
standards of supporting references.
Two-noted French doctors in their recent 900 page book "The Guide
to 4,000 Useful, Useless or Dangerous Medicines proves that “half of
France’s drugs are useless.” This is
what we get corporate tobacco ethic and
regulatory capture in our corporatist state. The subsequent article gives examples
of the process. As Prof. Angell
puts it:
“What can the 800 pound gorilla do; just about anything it pleases,” referring
to the $800 billion dollar industry. Hundreds of articles at www.healthfully.org confirm Angell’s
assessment.
TERMS:
Marketing
science, research done with the
objective of promoting their drug; distinguished from medical
science. Raw data
is the data
collected along with the conditions of a clinical trial. Science journals—except
medical) require
inclusion of the raw
data so the review committee can evaluate the article submitted; without it
review is a facade. Key opinion
leaders (KOL) are renowned specialists.
Their rise to prominence is based on consistently promoting pharma’s
goals and, for which most receive 6-digit income for services. KOLs are the
lecturers at continuing
educational classes, appear in the media, write textbooks, sign off on ghost
written journal articles, and are on guideline committees. Treatment
guidelines are pharma friendly standards of treatment issued by the FDA
& other organizations.
|
|
|
Key points (the business
norms): 1) The FDA has always been
headed by those with proven
track records, often executives from big pharma.[1] 2) The FDA creates
the façade of supervision
through their approval of drugs and subsequent regulatory actions such as
black-box warnings for serious side effects. This deception of protecting the
public is promoted by the corporate media. 3) The marketing departments of pharma control the
production of medical opinions: a) by funding 95% of large clinical trial pharma
decides what to study, trial procedures, and they own the results. b) They
always
manipulate published results. c) Pharma’s influences FDA-funded trials. d) Pharma creates the KOLs. e) Pharma
funds the mandated continuing-education
courses for doctors--$50 billion spent annually for sham education—twice
what they spend on research. f)
Pharma
provides half the funding of all health organization including the AMA, the
APA, & the American Heart Association. e) These organizations set up
treatment guidelines
that expand usages for drugs through relying on shoddy phase-4 clinical
trials. g) Litigious patients can
use
these guidelines in courts to claim malpractice. f) Sales reps (one for every 4 doctors)
establish a relationship with doctors to educate doctors. h) Doctors who push a company’s drug are
given perks
worth up to 6 figures annually. i) Direct-to-consumer ads create product
recognition and patient requests for them.
j) Low quality phase-IV clinical trials find new indications for their
drugs or to “prove” their drug is superior to off-patent drugs. k) KOLs
write pharma friendly textbooks. 4)
Administrators
of hospital, HMOs, and nursing homes receive through sales reps kickbacks
for setting up treatment
protocols using patented drugs[2].
5) Large perks are the norm for those doctors who favor one big pharma
company. Over 25% of pharma budget
goes
to influencing doctors, 14% to research.
Large cash reward for teaching and research is a powerful incentive. 6) Given
that bias is norm journals and
that 90% of articles on line require a payment of $35, doctors rely upon
guidelines & KOLs for guidance. We have pharma’s “expert”
based medicine. 7) For patent approval
by FDA, the drug must
be slightly better than nothing at all (placebo), and side effect are rarely a
reason for rejection. Half the drugs
aren’t worth their side effects. 8)
Since side effects reduce
sales, they are always grossly under reported.
8) Research
is market driven thus
treatment for chronic conditions are given priority over cures.
9) Instead of competing to make the best
drugs, all of big pharma use junk science and marketing techniques to hawk
their me-to-drugs (knockoffs). Less
than
10% of new drugs are innovative. This is what corporate tobacco ethics gives
us, and we pay for their marketing! 10) As Harvard Prof. Marcia Angell MD wrote:
“If we set out to design the worst system that we could imagine, we could not
imagine one as bad as we have”--her excellent President’s Lecture.
Supporting examples. 8) Most
drugs are tested on am ideal population and in real-world uses do
more harm than good. E.g., most cancer
drugs delay death in stage 4 (terminal) cancers by less than 3 months.
These drugs are then used for all stages of
cancer. The net outcome is to shorten
lives
of those cured by excision (without metastatic terminal cancer) because
of their side effects[3].
Blood pressure drugs suffer
from similar negative usage. 3) Bias in journal articles is the norm. In a study of 37 drugs for which the raw data
given the FDA became available through Freedom of Information Act to a group of
researcher, they found all the journal articles based on this research
exhibited a bias--between 11% and 69%, with an average of 32% (NEJM). This
entails that all published
clinical trials are biased. Thus
doctors
have can’t know what is best. Also
about
½ of clinical trials are not published This is equivalent
to flipping a coin ten
times and only reporting that there are just 5 flips, all of which are positive.
2 & 3) The FDA has done flawed studies with the intent of promoting the
sales of patented drugs. A prime
example
of this is the Women’s Health Imitative (2002) which the FDA knowingly used the
worst formulation of HRT, Prempro. Then
the FDA extended
Prempro results to all HRT formulas and warns that HRT has one
valid medical use, for hot-flashes, and it should be used at the lowest dose
for the shortest time. Natural HRT prevents osteoporosis,
Alzheimer’s, atherosclerosis, heart attacks, and colon cancer. Older journal
articles prove this.[4] Pharma profits from drugs for those
conditions. 2 & 3) FDA does
not require
head-to-head studies of drugs. When
pharma funds a comparative clinical trial of their drug (most often for
off-patent drug), it has been manipulated to “prove” theirs is superior—e.g. aspirin
cause more stomach bleeds, they
use a 2-pint transfusion for Plavix. 2) The combination
of marketing and other methods
listed above entail that a number of older, more effective off-patent drugs
have lost their market position. A
prime
example is that of diuretics
for high blood pressure (ALLHAT study). Their use has been replaced by the newer less-effective
patented drugs such as ACE inhibitors. 2) Basic medical science has been tweaked to
support sales. Heart attacks are
not
caused by high level of
cholesterol and hypertension,
rather by hardening of the
arteries caused by inflammation.
Giving a drug to lower blood pressure or cholesterol does not prevent
hardening of the arteries and subsequent pathology—numerous articles and books
prove the cholesterol myth. Pharma
used
the worst cases to show only very modest benefit from Statins based on flawed clinical trials.
2) FDA’s drug safety review is a
façade. They don’t
enforce either
the requirements to report side effects or to do a post-marketing studies on
side effects when requested. The
FDA licenses
worse-than-placebo medication including bisphosphonates (footnote),SSRIs, most cancer
drugs, ACE inhibitors, and Prempro. The most outrageous example that I have
uncovered are the selective COX-2 inhibitors. Vioxx
caused 125,000 heart attacks resulting in
55,000 deaths between 1999 to 2005; before it was voluntarily removed. They more than double the risk of heart
attacks, a fact exposed in 2001 in the VIGOR, &
the APROVE
Studies. Civil actions over the big 3 of COX2
inhibitors, Celebrex, Vioxx, and Bextra, resulted in over $3-billions civil
settlement. The gross disregard for public safety is why a number of
organizations critical of the industry (Worst Pill) recommend that patients use
older medications unless there is clear and convincing evidence that the newer
one is better. The FDA allows the
blockbuster
Celebrex; though other nations don’t. 6)
Pharma’s reduced usage of aspirin
by exaggerating risks, ignoring benefits[5] and promoting an ineffective low
82 mg dose, for which tolerance develops within a year. Aspirin prevents cancer through
apoptosis (death) of abnormal cells, effective treatment for arthritis, prevent
heart attacks, etc. thus the
assault upon aspirin. 2) Surrogate endpoints are used instead of cures
and life extension too often when the drug is useless, such as statins
and blood pressure drugs. They are
taken to prevent illness which they
do not. 8) Side effects are
dirty words, and there are numerous ways to under-report side effects,
including using healthy, young subjects, not including certain side effects in study
(e.g. reduction in libido from SSRIs is the norm), don’t quantify them but
include them in a list of over 20 side effects, trial period is too short for certain
side effects, such as cancer, no long-term follow up, to name some.
3) Ghost writing by pharma for
TV broadcasts & new articles for to promote drug sales. Journal articles, medical textbooks, etc. are
all pharma friendly.
Healthfully.org mission is to publish sound
evidence-based advice on drugs and treatments. This is an
arduous process. In 1980 I relied upon
my current edition of the pharmacology text book by Goodman and Gilman. Now
in the main, textbooks repeat pharma’s
bias, some are even ghost written by pharma.
Critics are still published in journals, I look for them. Much of my
research time is spent looking for
articles whose results are contrary to what pharma spouts. Animal and in vitro
studies fill the gap left
by pharma not wanting to expose a problem, such as Statins reduce CoQ10 by 40%. They are not pharma funded.
I look for bias in
abstract that are not supported in the article. Often I find glaring gaps in
information, which supports my suspicions.
Older articles, when there was still medical science, are of value, such
as on aspirin and HRT. A knowledge of
the biology behind a condition will often exposes marketing science. To sort
out bad science, hundreds or hours are spent on each topic published here. Often
the evidence for the bad drugs is
stronger than the positive alternatives.
The harm done by marketing entails that pharma should be limited to just
manufacturing.
[1]
Read the Consumer
Report article on the failure of the
FDA. “Pharma” means
drug manufacturers; “PhARMA” stands for their trade organization.
[2]
Bloomberg’s article on major
settlements over kickbacks; it
lists
J&J, Pfizer, Lily, AstraZeneca, and
Omnicare. It is the norm for the
industry.
[3] Lengthening
life a few months is not the same as saving lives from cancer; it fails to
measure total deaths or quality of life.
If the drug can’t cure a type of terminal cancer, then it can’t prevent
a stage 1-3 cancer from becoming metastatic, though pharma claims it.
[4] The prevalence of
osteoporosis is because women aren’t taking HRT which prevents bone
remodeling (loss).
Now women receive the class
of drugs called
bisphosphonates. They increase bone
density settling in the bones, but that doesn’t reduce bone fractures. Calcium loss can only be prevented by taking
natural estrogen
replacement, estradiol,—plant products don’t
work as well.
As of 1/27/14 on our don’t-take-list are
acetaminophen, anticoagulants, arrhythmia, bisphosphonates, hypertension drugs
other than diuretics, PPI inhibitors, NSAIDs other than aspirin, statins,
Alzheimer medication, and downers (psychiatric drugs that cause drowsiness).[1] On the take list is niacin, aspirin, natural
HRT, testosterone, and CoQ10--for the
evidence, 2-page updates. All chemotherapies should not be taken but for
only about 4 cancers that are curative
or capable of producing a remission
on average of over 2 years. For those without metastatic cancer they
significantly shorten life, and they won’t prevent part of a cancer missed from
following its natural course. If that
pieces missed is metastatic, then the patient’s fate has already been
sealed. If it isn’t metastatic, then
when it is later visible, it can be removed.
Chemo does more harm than good. The
side effects are serious. Alzheimer’s meds aren’t worth their side
effects. For most psychiatric conditions
behavioral therapy at 1 year out is significantly superior to drug
therapy. More drugs are added every
month. For nearly every condition for
which there is an effective treatment, the treatment is expanded to include
those who statistically don’t benefit. Pharma’s
performance is measured by profits, and profits have no conscience. Pharma has
co-opted the entire healthcare, regulatory, and information systems.
[1] Pharma has found many
indications for downers beside psychiatric conditions. Among them our nausness,
muscle relaxant,
post partum syndrome, pre-menstrual
dysphoric syndrome
|
|
|
|
|
|
|
|
A
gem: covers every major point in one
page.
http://www.bmj.com/content/346/bmj.f2695?ijkey=E4DHSRQzgZwTWOT&keytype=ref
Bad medicine: the way we manage diabetes
BMJ 2013; 346 doi:
http://dx.doi.org/10.1136/bmj.f2695 (Published 29 April 2013)
Cite this as: BMJ 2013;346:f2695
Type 2 diabetes is a modern plague largely
brought on by lifestyle and is considered a progressive, non-reversible
condition. The polypharmacy of chronic disease is the drug industry’s lottery
win, and no more so than in diabetes, with new drugs and the increasing use of
analogue insulin in type 2 diabetes worth tens of billions of pounds worldwide.1 ⇑
The
drug industry’s business plan for diabetes follows a familiar pattern:
·
(1) Conduct questionable
research and control the original data.
·
(2) Schmooze the
politicians, health regulators, and patient groups to suggest under-treatment
and need for “urgent action.”
·
(3) Recruit tame
diabetologists, massage them with cash, and get them to present at marketing
events that masquerade as postgraduate education.
·
(4) Pay doctors to switch
to newer drugs in dubious international post-marketing “trials.”2
·
(5) Seek endorsement from
the National Institute for Health and Care Excellence to bully doctors to treat
diabetes aggressively with drugs.3
And
so the complexities of diabetes are reduced to simply lowering blood sugar.
What is the annual cost of pursuing this
reductionist, drug based approach? In the past decade, spending on insulin in
the UK has risen 300%, to £311m4 (€356m; $463m), and on
oral diabetic drugs 400%, to £277m. And have you ever wondered why companies
generously give away glucose meters? Test strips are a £166m market, the value
of which has risen 300% in 15 years.4 Factor in staff time
(when not attending more educational updates sponsored by the drug industry)
and the patient and family’s time, and you have a great but expensive business.
But do analogue insulins, new diabetic drugs,
and self monitoring of blood glucose improve outcomes? Does even tight
glycaemic control make a difference? No data on mortality or morbidity exist
for the new therapeutics.5 6 7 8 9 10 11 Likewise intensive
glycaemic control is not superior with respect to mortality and cardiovascular
disease.12 So billions of pounds
are being spent chasing a ghostly surrogate endpoint: low blood sugar. Worse,
there is evidence that these new drugs cause harm. Rosiglitazone has already
been withdrawn; pioglitazone has been linked to bladder cancer; and exenatide
and sitagliptin double the risk of acute pancreatitis.13 14 All this is an example
of the scientific illusion that is so called evidence based medicine, where
research is just mechanically reclaimed statistics pulped into junk educational
nuggets—mere marketing by another name. There
remains another fundamental question. Can diabetes be reversed or cured by
weight loss? A small, well designed study of 11 patients irrefutably showed
that it can.15 And clinical effect is
more important than any statistically significant yet clinically undetectable
effect that a huge study funded by the drug industry might find. The
therapeutic approach in diabetes is upside down. Incredibly, spending on
diabetes drugs could employ 40 000 personal trainers. The complicity of doctors
and lack of dissent against the drug model of diabetes care is bad medicine.
Notes
Cite this as: BMJ 2013;346:f2695
Footnotes
·
Provenance
and peer review: Commissioned; externally peer
reviewed.
·
Follow
Des Spence on Twitter @des_spence1
References
1. ↵
Cohen D, Carter P. How small changes led to big
profits for insulin manufacturers. BMJ2010;341:c7139.
FREE Full Text
2. ↵
Gale EA. Post-marketing studies of new insulins:
sales or science? BMJ2012;344:e3974.
FREE Full Text
3. ↵
National Institute for Health and Care
Excellence (NICE).
Blood-glucose-lowering therapy for type 2 diabetes. April 2013. http://pathways.nice.org.uk/pathways/diabetes#path=view%3A/pathways/diabetes/blood-glucose-lowering-therapy-for-type-2-diabetes.xml&content=view-node%3Anodes-considering-triple-therapy.
4. ↵
Health and Social Care Information Centre.
Prescription Cost
Analysis—England, 2012. April 2013. www.hscic.gov.uk/catalogue/PUB10610.
5. ↵
Davidson MB. Counterpoint: self-monitoring of
blood glucose in type 2 diabetic patients not receiving insulin: a waste of
money. Diabetes Care2005;28:1531-3.
FREE Full Text
6. ↵
Horvath K, Jeitler K, Berghold A, Ebrahim SH,
Gratzer TW, Plank J, et al. Long-acting insulin analogues versus NPH insulin
(human isophane insulin) for type 2 diabetes mellitus. Cochrane Database Syst Rev2007;2:CD005613.
Medline
7. ↵
Van de Laar FA, Lucassen PL, Akkermans RP, Van
de Lisdonk EH, Rutten GE, Van Weel C. Alpha-glucosidase inhibitors for type 2
diabetes mellitus. Cochrane Database Syst Rev2005;2:CD003639.
Medline
8. ↵
Shyangdan DS, Royle P, Clar C, Sharma P, Waugh
N, Snaith A. Glucagon-like peptide analogues for type 2 diabetes mellitus. Cochrane Database
Syst Rev2011;10:CD006423.
Medline
9. ↵
Black C, Donnelly P, McIntyre L, Royle PL,
Shepherd JP, Thomas S. Meglitinide analogues for type 2 diabetes mellitus. Cochrane Database
Syst Rev2007;2:CD004654.
Medline
10. ↵
Richter B, Bandeira-Echtler E, Bergerhoff K,
Clar C, Ebrahim SH. Rosiglitazone for type 2 diabetes mellitus. Cochrane Database Syst Rev2007;3:CD006063.
Medline
11. ↵
Ooi CP, Loke SC. Colesevelam for type 2 diabetes
mellitus. Cochrane Database Syst Rev2012;12:CD009361.
Medline
12. ↵
Hemmingsen B, Lund SS, Gluud C, Vaag A, Almdal
T, Hemmingsen C, et al. Targeting intensive glycaemic control versus targeting
conventional glycaemic control for type 2 diabetes mellitus. Cochrane Database Syst Rev2011;6:CD008143.
Medline
13. ↵
British National Formulary (BNF). www.bnf.org/bnf/index.htm.
14. ↵
Singh S, Chang HY, Richards TM, Weiner JP, Clark
JM, Segal JB. Glucagonlike peptide 1-based therapies and risk of hospitalization
for acute pancreatitis in type 2 diabetes mellitus: a population-based matched
case-control study. JAMA Intern Med2013;173:534-9.
Medline
15. ↵
Lim EL, Hollingsworth KG, Aribisala BS, Chen MJ,
Mathers JC, Taylor R. Reversal of type 2 diabetes: normalisation of beta cell
function in association with decreased pancreas and liver triacylglycerol. Diabetologia2011;54:2506-14.
CrossRefMedlineWeb
of Science
^^^^^^^^^^^^^^^^^^^^^^^^
From Worstpill.org: A recent
article in the British Medical Journal by
a Scottish general practitioner
reminded me of a book about diabetes pills that we published 35 years ago
telling much the same story…. When our book Off Diabetes Pills was published in 1978, none of the
diabetes pills available in the U.S. had evidence, beyond lowering blood sugar,
of a positive effect on mortality or a reduction in cardiovascular disease… A
major reason for our writing this book was that back in the 1970s, there was
already some evidence of harm from oral diabetes drugs. Since then, the number
of harmful diabetes pills has greatly increased, with several so dangerous they
had to be banned. These included phenformin, which caused often-fatal lactic
acidosis, and troglitazone, which caused frequently fatal liver failure. Most
recently, the widely used
rosiglitazone (AVANDIA) was banned in Europe in 2010 due to increased
cardiovascular risk, including heart attacks and heart failure. Worst
Pill
The point of taking a drug
is improvement of life quality. To
change a surrogate end-point, blood glucose without improving health or
extending life is a hollow victory. To
do so with risk of serious side effects, expense, and inconvenience is a bad
choice. For how had PhARMA is, please
read http://healthfully.org/rc/id1.html
and http://healthfully.org/rc/id9.html
--jk
INTERNAL SITE SEARCH ENGINE by Google
Looking for a topic, use Google Internal Search
Engine
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^ Remember that
pharma is in the business of treating illness. There claim of preventing illness is in most cases mere marketing.
Disclaimer: The
information, facts, and opinions provided here is not a substitute for
professional advice. It only indicates
what JK believes, does, or would do. Always
consult your primary care physician for medical advice, diagnosis, and
treatment.
|
|
|
