|

Saturated
fats and monounsaturated
fats are the
best sources to replace the energy from carbs.
CoQ10 (Q10),
which is found in every cell in the body, should
be taken daily starting in
the teen years; it is the best of the fat soluble antioxidants. In addition
women starting with menopause and
continuing thereafter should take the natural HRT (estradiol
and progesterone available only from a compounding pharmacy), and men starting
between 60 and 70 should take testosterone at a high
dose available from a compounding pharmacy. There is 50% reduction in MI with
estradiol;
it lack is why cardiovascular disease and heart attacks occur following
menopause. Men on Testosterone are will exercise more,
less likely to develop metabolic syndrome (diabetes, hypertension, obesity, and
AS), and are more likely to survive
an MI. Both hormones have numerous other
healthful benefits such as the prevention of osteoporosis. For these reasons
KOLs instruct doctors against the use of hormones. Aspirin in the anti-inflammatory dose of 325 mg with meals
prevents atherogenesis, cancer, Alzheimer’s disease, and numerous other conditions. Thus
pharma runs
junk clinical trials and then educates doctors to warn patients of the risk of
ulcers, though the risk increase is minor.
The perverse outcome is because all the other NSAIDs recommended by
physicians increase the risk of heart attacks—significantly enough for the American Heart Association to issue a clear warning. I’d rather double the risk of an ulcer, than not
lower the risk of the much more common heart attack by 50% and cancer by over
30%. Aspirin, estradiol, and Q10 along with
healthful lifestyle and low carb-sugar diet can stop the formation of new plaque, and thus over
the next
4 years will greatly reduce the risk for heart attack and stroke as the body
stops making young unstable plaque, the cause of over 85% of heart
attacks.
| Figure A should be swollen and partially ocluded, |
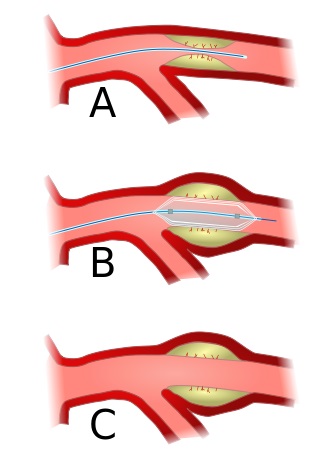
|
| See more acturate representation top of page |
You might wonder how the system
could become this
broken, and yet go under the radar of opinion.
The short answer is that advertising and propaganda works. How did the
Nazi party gain overwhelming
popular support. How can people support
the world popular religions given their mythic foundation? The list of dumb
beliefs and actions is
long. Add to this the faith in
pharma. A confluence of corporate moves
has created the collection of treatment myths.
Pharmaceutical corporations should not be doing research, owning the
results including raw data, controlling its publication, give continuing
education to physicians taught by pharma’s KOLs,
head the FDA, influencing treatment protocols (guidelines), and misinforming
the public about drugs on television and through physicians who are taught by KOLs.
Forty years ago, medical text books did a reasonable good job of
providing information; that has all changed, since they are written by pharma’s
KOLs. Before Regan’s Presidency,
clinical trials
were ran by universities, now pharma is involved in all stages of clinical
trials, often through corporations whom they hire to run the trials and right
the journal articles. Their influence in
universities over research determines who becomes key opinion leaders (KOLs)
and thus write textbooks. Ghost
writing has become the norm for clinical trial.
The extent of intrusion has been meticulously documented in Prof. Ben
Goldacre’s Bad Pharma. Harvard
prof. Marcia Angell has an equally excellent book on How Pharma deceives us. There is a fundamental conflict between
short-term profit maximization and the public’s health, I call this tobacco
ethic. The articles written for
the recommend section of healthfully.org make adjustments for the marketing
distortions of pharma. A quality study
of 74 published articles comparing raw data to published results determined
that positive bias
averages 32%. Thus what seem to
work based on the published evidence base, in the vast majority of cases
doesn’t. And it gets worse because side
effect weren’t considered—how could they given the reporting system is
broken. Healthfully.org/rc adjust for our broken system and thus provides
the information for informed choices in the best patient’s interest. As
of November 2014, 18 areas of treatment
and drugs have been published. An
important new section is on diet and its role in CVD, metabolic
syndrome, and obesity. These articles
are regularly updated. In that new section are links to a number of on-point YouTube videos. Included
there are videos on bad pharm, SSRIs, cholesterol myth, the use of statins,
diet, and diabetes—and there are books listed.
Unfortunately there aren’t quality
videos on exposing hypertension, arrhythmia, acetaminophen, anticoagulants,
chemotherapy, bypass operations, polypharmacy, SSRIs, Nor are there quality
videos on the health
benefits of aspirin, CoQ10, and hormones, but there are books on their
benefits.
|
Two essential points are essential for
understanding why the recommendations below are contra pharma’s
position. One that pharma has tobacco
ethics, the rule by which corporations function to maximize profits. Second,
applying this rule, they do all
that is necessary to promote
their patented drugs, and to reduce the usage of off-patent
drugs and drugs which would prevent chronic conditions. Research
is done for marketing goals, thus bias
is the norm. The drugs listed below have a compelling
body of evidence published at /rc ,
diet at /rh. Examples of their tobacco ethics is at bad
pharma and at /rep which is a
collection of critical journal articles.
There are links to a collection of the best of university lectures and
documentaries on the issues
raised.
|
HEALTHFUL CHOICES
Lifestyle
makes a difference:
The greatest gains are from weight
control, low-carbohydrate-sugar diet, cessation of smoking, and vigorous
exercise.
Rapping the heart in a layer of fat and making the heart pump harder
through miles of blood vessels are consequences of obesity. Moreover with obesity, adipose tissue affects
the feedback mechanism that regulates insulin; thus the risk of type-2 diabetes
increases by 30 fold. Diabetes causes
a
higher level of blood borne sugars increases the rate which accelerates
glycation. Diabetes causes red blood
cells to leak out of capillaries which cause an immune response by
macrophages. For these reasons diabetes
doubles the rate of MI. Diabetes shortens life an average of 5 years
and with obesity more. The carbon
monoxide--a reactive chemical that damages LDL-- from tobacco doubles the rate MI.
A pack-a-day smoker shortens their life on an average 12 years. Carbon monoxide promotes the production of
unstable plaque, thus with cessation, the risk for MI dramatically drops over the next 5 years. Vigorous
exercise
strengthens the heart, better vascularization, & has anti-inflammatory
effect thus and healthful
effects
upon the epithelium (cell walls) of arties. Controlling for lifestyle contravening
variables, senior runners extended life 8.7 years, & it improves quality of
life. “Exercise capacity
is a powerful
predictor of mortality” NEJM.
Diet makes a difference, but not the diet that
pharma & our government teaches which promote the fat-cholesterol
myth. In 11 out of 12 studies reviewed in Wikipedia,
results did not have a benefit from low fat, or increased ratio of
polyunsaturated fats “A meta-analysis of 21 studies considered
the effects of saturated fat intake and found that Intake of saturated fat was
not associated with an increased risk of CHD (coronary heart disease), stroke,
or CVD (cardiovascular disease)" Wiki. The initial cause of CVD is damage to LDL caused by sugars and by reactive
chemicals. Sugars
damage LDL
through glycation where the monosaccharide attaches to the LDL.
A high sugar diet (especially fructose) is
associated with insulin resistance (high blood sugar level), diabetes, and
metabolic syndrome; all are causal factors for AS. Fat as stated before
is
not the culprit: “Indeed, recent prospective cohort studies have not
supported any significant association between saturated fat intake and
cardiovascular risk” BMJ. Instead, saturated fat has been found to be protective.
Trans-fats and high ratio of omega-6 to omega-3 fatty
acids however promote CVD. However,
in
most countries trans-fats are effectively banned (not the US), and the ratio of
the omega 6 acids can be reduced by decreasing the use of vegetable oils with
the exception of coconut oil.
Aspirin: “Irreversibly blocks
the formation of thromboxane A2 in platelets, producing an inhibitory effect on platelet aggregation. This antithrombotic property makes
aspirin useful for reducing the incidence of heart attacks.[113] ”[114]
Since platelets have no DNA, they are unable to synthesize new PTGS once
aspirin has irreversibly inhibited the enzyme, an important difference with
reversible inhibitors…. aspirin induces the formation of NO-radicals in the
body, which have been shown in mice to have an independent mechanism of
reducing inflammation.” Wiki. The platelet effect reduces thrombosis risk over 40% (with
325 mg) and the NO (nitrous oxide) in slowing/preventing atheriogenesis. Atherogenesis
slowed: “strong evidence that
atherosclerosis is slowed down in a dose term … aspirin,” and
stopped. This effect is
dose dependent, comparing
900 to 50 mg of aspirin. At 325 mg with
meals aspirin has an anti-inflammatory
effect and thus prevents
the formation of young unstable plaque, the cause
of ischemic events. Benefits; Various
mechanisms: By NO endothelial cells
from
oxidative
damage, inhibits leukocyte
attacks, cytokinies, & CD36. The anti-inflammatory effect has other healthful
consequences. Also prevents cancer
and cures it by
stimulating the body’s necrosis factor.
And has other
benefits. The risk of bleeding is
greatly exaggerated by pharma
who opposes prevention of chronic conditions through their numerous marketing
clinical trials and use of opinion leaders to instruct physicians in their
required continuing education classes (the same has been done with estrogen). The increased risk of major bleed with
aspirin long-term is 4%.
Estradiol
with progesterone (natural HRT): Estrogen is why women prior to menopause don’t
have cardiovascular disease. Estrogen
lowered by 20% cholesterol, 37% LDL (bad cholesterol) and raised by 14% HDL 14%, extends life 2.1 years, Braunwald,
Heart Disease …, 5th Ed, 1997, p 1708 tables. “Estrogen-replacement therapy decreases
CAD morbidity and CAD mortality … was 0.56
compared to subjects not taking estrogen” [a 44% reduction] Braunwald supra
1142. Another study found a 50% reduction in CHD.
Estradiol blocks
oxidation of LDL to prevent
atherosclerosis. “Estradiol completely reverses the effects induced by
OX-LDL on the DDAH/ADMA/NO pathway,” Avoid MPA and LNG (levonorgestrel). Another study found 26 deaths for estradiol vs. 56 for placebo. A meta-study found and a 50% reduction of Coronary Heart Disease.
AHA study explains
mechanisms of cardio protection. Angina pain (cardiac
syndrome X) associated with low estrogen, treated. Estradiol
plus progesterone for CVD & death is the best HRT. Other benefits of
natural HRT: the prevention of
osteoporosis, Alzheimer’s disease, colon cancer, and arthritis.
Testosterone: Prevents metabolic
syndrome MetS (poor cholesterol profile, obesity, and high blood pressure): “Emerging evidence suggests that testosterone therapy
may be able to reverse some aspects of metabolic syndrome” And another. “These
results suggest that low SHBG [sex hormone-binding globulin] and/or AD
[androgen deficiency, TTT] may provide early warning signs for cardiovascular
risk and an opportunity for early intervention in non-obese men.”
In a matched study
followed ten years published by the AHA
found that the lowest quarter of men were 41% more likely to die from
cancer and cardiovascular disease compared to the highest quarter. Low
TTT
is associated with
cardiovascular disease. TTT Inhibits
atherogenesis: in a survey paper, “Positive correlation between total or free
testosterone level and HDL and a negative association the LDL” and. Conclusion: “A normal physiological level
of TTT in men protects against the development of high cholesterol, insulin
resistance, hypertensions, clots that
cause heart attacks, obesity, and increased waist:hip ratio, all of which
predispose to the development of CVD.
Low or low normal TTT is implicated in the pathogenesis of acute MI and
acute stroke. The decline of TTT with
age may explain the greater risk of CVD with advancing years” [medical
terminology simplified by jk]. TTT is
good for your heart, muscles, and blood vessels. Heart Attack, after
controlling for factors low
TTT
associated with
MI,
positive effect upon fibrinolytic
pathway, reduces
angina.
Coenzyme
Q10 (CoQ10, Q10): For heart failure (HF): the heart isn't
able to adequately pump blood, thus it pools in parts of the body, such as the
lungs and legs. “Several
clinical studies suggests that Q10 supplements
help reduce
swelling in the legs; reduce fluid in the lungs to making breathing easier; and
increase exercise capacity in people with heart failure, and reduces hospital admissions
by 61%”,
similar, also,
long-term
and safety.
After Heart Attack and Angina
pain: A clinical
study found that
people who took daily CoQ10 supplements within 3 days of a heart attack were
less likely to have subsequent heart attacks, less chest pains, die of heart
disease. The capacity
for exercise improved
about 30%
for those with chronic heart failure on taking Q10, also. High
blood pressure: In a meta-analysis
of 12
clinical studies,
Cochrane concluded that Q10 lowers systolic blood pressure by up to 17
mm Hg and diastolic blood pressure by 10 mm Hg, probably from improved heart
functions. Bad cholesterol: Q10 attaches to LDL. It reduces oxidative
damage
and thus slows atherogenesis.
The
mitochondria produce ATP, the energy source for nearly all bodily
functions. Q10 protects the mitochondria
from oxidative damage, and thus will very significantly improve, when taken
long term, endurance for those over 60 years.
The decline in function of the mitochondria is the reason for the
dramatic drop in endurance of the elderly.
More ATP entails that the elderly are more likely to survive an MI. For
this anti-oxidant effect in the
mitochondria and upon atherogenesis, Q10 should like vitamins be taken life-long. There
are numerous other benefits including
improving blood sugar level in diabetics, for Parkinson’s disease, migraines,
and macular degeneration, and it should be used with statin therapy, since
stains partially block Q10 production.
|
There is a large body of clinical
trials and epidemiological studies that have shown that cholesterol and high
fat diet have minimal effect upon promotion of CVD, and conversely that a low
fat & low cholesterol diet is not cardiovascular protective (see Cholesterol
Myth). As stated prior reactive chemical damage to
LDL (especially glycation) and the immune response is the primary cause, thus
drugs listed below and low sugar diet have significant effect while Statins
for an assortment of reasons are not worth taking. Since so many believe in
the cholesterol
myth, the natural, safer method of lowering blood cholesterol with niacin and
its inositol form are included below.
|
Niacin
improves
cholesterol profile by
lowering of plasma triglycerides mobilization
from adipose
tissue, and inhibiting hepatocyte diacylglycerol acyltransferace synthesis of
triglyceride thereby lowering cholesterol and thus “inhibits the synthesis of
apo-lipoproteins and the influx of free
fatty acids (FFA) into the
liver, which is the precursor of triglycerides.” “A single dose
of niacin 200 mg given in the
fasting state [at bedtime] provides a
prompt and marked fall in serum FFA
level, with a rebound after some hours. A
comparable fall in plasma FFA occurs
normally following a carbohydrate-containing meal, when adipose tissue
lipolysis [making lipoproteins] is
inhibited by insulin, and re-esterification of FA in adipose tissue cells is
increased by glucose. Therefore,
the FFA level is usually low during
the day, when carbohydrates are the predominant source of calories [thus
preventing a niacin caused reduction in FFA].
Lipolysis becomes active in
the post-absorptive state at night, when the FFA-level
is approximately double the daily mean level. “Oral
administration
of niacin … during the day does not
appreciably alter this pattern.” This is
why blood cholesterol blood work requires fasting, and why niacin and IHN should
be taken at night, when the
insulin level is low. Thus a low dose at night-- 200 to 500 mg--is sufficient. Plasma
peak is for niacin 30 minutes, half life under 1 hour. This entails rapid absorption
and excretion during a time when it is ineffective because of low level of
FFA. Pharma’s
recommendation of a mega dose of niacin (ignores INH) creates very low
compliance due flushing, and during the day for minimal effectiveness. This
pattern of marketing first is the norm
for Pharma.
Inositol hexanicotinate (IHN, a source of niacin): The
literature is thin, since Pharma members won’t research a flush-free, effective
treatment for high cholesterol. Though IHN
releases niacin, it does at too low a rate to affect the same
bio-pathway as niacin (peak for Niacin is 45 minutes, IHN 8 hours). (A criticism
by Pharma of INH, but shown
false in a quality study using blood samples drawn at night). INH
affects Free Fatty Acids (FFA), rather than lipolysis as does niacin and
statins. “FFA
is a precursor
of plasma triglycerides. Lipolysis becomes active in the
post-absorptive state at night, when the FFA-level is
approximately double the daily
mean level…. The Xanintol
esters and IHN were superior at lowering FFA,” at Eur.
J. Clin.
Pharmacol. 16, 11-15 1979. In another
study “At 6 weeks of usage [1650 mg IHN] found a
nearly 20% improvement in cholesterol profile”. Given a bio-pathway not effecting CoQ10 (as
does statins and niacin), on thin evidence jk recommends INH over niacin.
Hypertension:
Hypertension is a
result of atherosclerosis, thus lowering blood pressure has little effect upon
ischemic events. The best approach is to
prevent formation of young unstable plaque and thus atherogenesis. Start with
lifestyle changes of exercise, weight control, healthful diet low
in salt and saturated fats, Q10, and use of aspirin, hormone replace if
suitable, and see if that brings it to a safe level within 2 years, systolic
under 180 and diastolic under 110.[1] Blood pressure will drop slowly. Moreover fluctuation during the day is
significant, and dependent on situation when taken. Relax when blood pressure
is taken; it will
reduce systolic pressure by at least 10.
“One study found that 41% of
patients 50 and older who were carefully taken off their high blood pressure
medications did not need them, having normal blood pressure 11 months after the
drug was stopped”18
Worst Pill. “Only
the thiazide and loop diuretics have good evidence of
beneficial effects on important endpoints of hypertension, and hence, should
usually be the first choice when selecting a diuretic to treat hypertension. They
are the recommended as first-line
treatment in the US (JNC VII) [5] and European (ESC/ESH) [6] guidelines…. Thiazide diuretics also increase calcium
re-absorption at the distal tubule” Wiki. Thiazides are
“associated with an increase in bone mineral density and reduction in fracture
rates attributed to osteoporosis” Wiki. And their cost
is
under $100/year. Pharma to promote their
drugs distorts the pathology cause of primary hypertensions (90% of
cases). It is the same as that which
causes CVD, atherosclerosis, namely
clogged, stiff arteries. Pharma pushes 8-families
drugs all of whom but diuretics aren’t worth the side effects.
RECOMMENDATIONS FOR HEALTH: Healthful
lifestyle of normal weight, diet low in salt and sugar, and regular
exercise. For those with CVD or
cholesterol above 280 or blood pressure systolic above 180 (markers for CVD)
325 mg of aspirin with each meal for its anti-inflammatory effect. For
everyone because CoQ10 is an
effective anti-oxidant in found in LDL thus reducing atherogenesis and it
protects the mitochondria from oxidative damage, the reason for age related
decline in peak athletic performance and physical endurance. Given Q10’s
safety and benefits, I would give
it to children (atherogenesis is present in all children). Aspirin 325 mg lowers
risk of ischemic event and increases survival of cancer over 40%, plus MI by
30%, and prevents atherosclerosis. Testosterone lowers risk
of MI, heart failure, and metabolic syndrome.
Estradiol is why women don’t develop cardiovascular disease until after
menopause. If systolic blood pressure
remains above 160 after 2 years of doing what has been recommended, then try a
low dose thiazide (see section above). Read Marking Science, and Junk Treatments, and be skeptical of medical
(marketing) “wisdom” and physicians whom have been co-opted by corporate
medicine. Thus avoid their push for
polypharmacy: statins, blood thinners,
hypertension drugs, arrhythmia drugs, and drugs with cognitive side effects
(downers dressed in drag). Doctors are
very good at impressing patients with sophisticated tests, scare tactics, and
magic bullet drugs that affect a specific bodily process, while they are
fulfilling a pharma-friendly protocol, all supported by market science. Memorize
the words of Harvard Prof.
Dr. Marcia
Angell: “We
certainly are in a health care crisis, ... If we had set out to design the
worst system that we could imagine, we couldn't have imagined one as bad as we
have.” Author of the Truth About Drug
Companies, and former Editor in Chief of NEMJ.
Put another way: “The
pharmaceutical industry is the most lucrative, the most cynical and the least
ethical of all the industries," and watch her lecture on YouTube.
Dr. Philippe Even tells The Guardian.
"It is like an octopus with tentacles that has infiltrated all the
decision-making bodies: world health
organizations, government agencies, parliaments, high administrations in health
and hospitals and the medical profession." JK
from 1991 to 1996 took 2.5 gm of aspirin for chronic
back pain, and 325 thereafter, daily exercise since 1974, and 5 gm daily of
nutritional yeast (source of niacin) sprinkled on foods since 1981,
testosterone from a compounding pharmacy since 2003—his total cholesterol is 165
and blood pressure 125 over 73, BMI of 21, and he is in his 7th
decade, and he doesn’t get heart burn.
^^^^^^^^^^^^^^^^^^^^^^^^^^
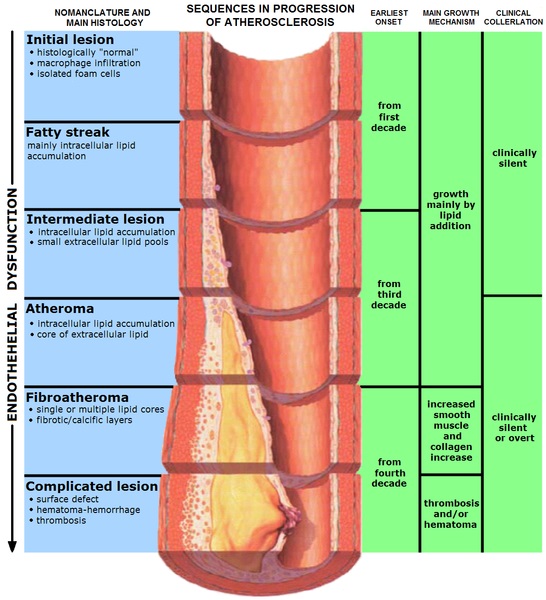
Non-technical summation
Hardening of the arteries (atherosclerosis, cardiovascular disease): Cardiovascular disease results from reactive
chemical damage (especially glycation from sugars) to LDL and VDL (the bad
cholesterols) that stimulates an inflammatory response in macrophages (a type
of white-blood cell). They ingest the
damaged LDL. When too much they become
foam cells that die to form plaque within the walls of arteries that when
sufficient become the medical condition of atherosclerosis. Leaking plaque
cause over 80% of strokes and heart
attacks.. Healthful
life-style of
low carbohydrate-sugar diet and exercise are the
first line of defense. CoQ10 should
be taken daily starting in the teen years.
In addition women starting with menopause and continuing thereafter
should take the natural
estrogen (estradiol), and men starting between 60 and 75
should take testosterone. There is major
cardiovascular protection with estradiol; it is why cardiovascular disease and
heart attacks occur following menopause. Men on Testosterone
are less likely to develop metabolic syndrome (diabetes, hypertension, and
atherosclerosis) and are more likely to survive a heart attack. Estrogen and
Q10 protect LDL and VDL from reactive
chemical damage, and aspirin and estrogen inhibit the inflammatory
process. As for Statins: pharma
hypes its benefit and hides their side effects. Lowering cholesterol has no
significant effect
upon atherogenesis. Aspirin, however, in
the anti-inflammatory dose of 325 mg
with meals or greater prevents atherogenesis, cancer, Alzheimer’s disease, and numerous other conditions. Thus
pharma runs junk clinical trials and educates doctors not to recommend an effective
dose of aspirin. Aspirin, estradiol, and
Q10 along with healthful lifestyle and low carb-sugar diet can stop the formation of new plaque, and in
most cases over the years there will be a gradual lowering of risk for heart
attack and stroke as the body heals through revascularization.
|