|
KEY POINTS: Everything your
doctor has learnt
about CVD is a product
of pharma-generated
tobacco science. What medical science
has uncovered about CVD. CVD is synonymous with
atherosclerosis, a process where the artery walls are damaged by the
accumulation of plaque (atheroma). “An atheroma is an accumulation of degenerative material in the tunica intima (inner layer) of artery walls.
The material consists of (mostly) macrophage cells,[1][2] or debris, containing lipids (cholesterol and fatty acids), calcium and a variable amount
of
fibrous connective tissue” Wiki. The cause of the plaque formation is an
inflammation response by white blood cells (macrophages) and LDL to the presence
of pathogens within the tunica intima (layer just below the endothelium). Yes,
LDL has two functions, one of transport
of cholesterol and triglycerides, the other in the immune system, it contains
on its surface antibodies. The role of
pathogens was accepted more than a hundred years ago.[1] The LDL and white blood cells are actively
transported by the endothelia cells that line the artery was as a response to the pathogen. If
the immune system can destroy the pathogen
then no puss like atheroma will form. If
not then the wall of the artery will expand due to the accumulation of plaque. A
number of factors can promote this
process. Since the endothelia cells act
as a barrier to pathogens circulating in the blood, various chemicals which
diminish the function of those cells increase the risk of infectious
invasion. Among those are reactive
chemicals circulating in the blood, of which carbon monoxide and fructose are
the most clinically significant. Tobacco
smoke and a high sugar diet are the major sources. Fructose also contributes
through a process
in which it is converted to fat and stored in the liver, thereby resulting in
metabolic dysfunction of which insulin resistance is one consequence. Fatty
liver is a result of the combination of
sugar (fructose) and glucose mostly from starches-- both are consumed in excess
by those eating a Western diet. (CVD is nearly unknown among the
elderly populations that eat a hunter-gatherer—paleo—diet.) The
effect of the Western diet upon the
immune system also contributes, as does drug which compromise immune
functions—see NASIDs. Another causal factor is chronic infectious
conditions such as gingivitis. Pharma
makes billions treating the fake causes and the consequences of CVD.
A
cutting edge
restatement of the
above causes of cardiovascular disease (CVD) from a 2009 Journal
article: “Atherosclerosis is now recognised
as a chronic
inflammatory disease occurring within the artery wall and ultimately
responsible for myocardial infarction, stroke and peripheral vascular disease.
A crucial step in
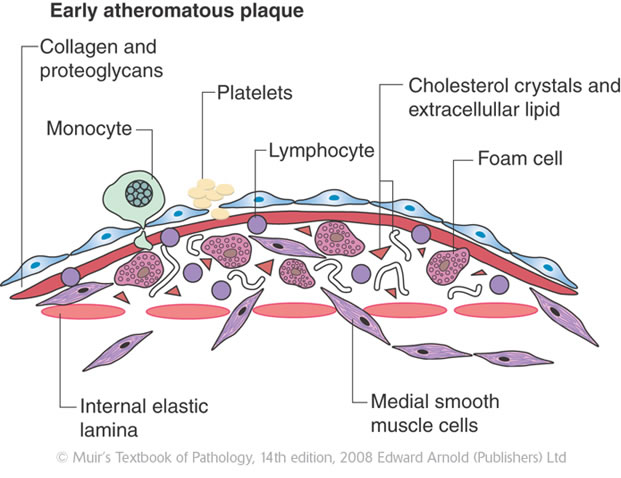
atherogenesis is the infiltration of monocytes[2]
into the sub-endothelial space of large arteries where they differentiate into
macrophages and become functionally active. Macrophage[3] accumulation within plaques is a hallmark
of all
stages of atherosclerosis, indeed recent
studies have shown their presence has the potential to act as a non-invasive
marker of disease activity and plaque stability. Activated macrophages are major
players in all
stages of lesion development. They not only accumulate lipids but also express
effector molecules that are pro-inflammatory, cytotoxic and chemotactic.
Furthermore, they secrete enzymes that degrade extracellular matrix leading to
plaque destabilisation and increased
risk of rupture. However, macrophages are heterogeneous and when
appropriately activated they have the potential to drive tissue remodeling and
ultimately vascular repair. Pharmacological modulation of macrophage activities
therefore represents an important strategy for the prevention and treatment of
atherosclerosis and other inflammatory diseases.”
So
what is the
main cause of the immune response? “Glycation of LDL
occurs chiefly due to the non-enzymatic
reaction of fructose [glycation] and its metabolites with the free amino groups
of lysine in which LDL is rich. There is generally more
circulating glycated LDL than oxidatively modified LDL….
Both prevent LDL receptor-mediated uptake and
promote macrophage scavenger receptor uptake. The recognition that LDL glycation is at least as important as oxidation
in atherogenesis…” The wrong causal model--that of cholesterol plugging up arteries--entails poor results. The drug to
lower cholesterol in LDL
transport, statins, in the early clinical trials proved that lowering
cholesterol had no effect upon the endpoint of death”.[4] The later trials didn’t meet scientific standards. Why
does this false theory of
high LDL, cholesterol, and triglycerides persist? See appendix at bottom for
a brief discussion
and read Prof. Uffe Ravnskov’s book Ignore the Awkward! It is one of the 2 best on the
Cholesterol Myths, and it has a section on the real cause.
Dietary
cholesterol causes clogged arteries:
In 1913 Nikolai
Anichkov (Russian) fed rabbits
cholesterol and showed that it caused atherosclerosis (but rabbits are
herbivores).
Propter and Gamble in marketing
their hydrogenated vegetable oil, Crisco, latched on this experiment to promote
the idea that vegetable fats don’t cause CVD.
Using bad science generated by the food industry, bad government ran
with the myth that a high fat diet causes CVD, and added to it the cholesterol
(see Part 2).
It was in an era of unrestricted use of the blood vessel clogging
unnatural transfats—clogging because the body lacks an enzyme for its
metabolism. These transfats are still
common because of pseudo government regulations. Some European countries totally
ban transfats
(see Part 4).
Part
3 explains the greater role of
carbohydrates especially fructose in obesity and CVD. Part 4 goes into the fat myth and also
reviews the evidences on the good and
bad fats. Part 5 is on diet and healthful
choice. Part 6 is on the diet vector
in illnesses and dietary fixes. And Part 8 deals with the second deadly
specter, the obesity epidemic. And there
is a posting on the Atkins
diet with JK’s improvement. A
search of the site using the internal Google search engine will uncover
articles to answer most questions.
So why doesn’t pharma
market drugs to prevent AS? Pharma in their business model has 3
principle reasons: 1) there are no drugs
that remove the plaque which is inside the artery tunica intima.[5] 2)
To promote drugs that would prevent or slow
atherogenesis would reduce the sales of drugs to treat hypertension (HT),
prevent blood clots, arrhythmia, and high TC[6]. The drugs that prevent AS also
reduce the risk of developing those chronic conditions, and thus would lower
pharma’s profits by 50% within a generation (see part 4). 3) There are 4
drugs which significantly lower the risk of developing AS, but estradiol
and testosterone are off-patent drugs, and the other two are over-the-counter,
325 mg aspirin and CoQ10. Moreover, these drugs as a group greatly reduce the
risk of
blood clots, cancer, Alzheimer’s disease, osteoporosis, acute ischemic events, HT
and other diseases. Thus they
do tobacco science to protect
profits. And it gets worse, since the
best preventive treatment is a healthful diet.
Pharma treats TC with one
of
their 10 statins and HT with three from their over 120 drugs, which come
in 7 categories based on method
of action. A patient who is in the high
risk group for an ischemic event
is also placed on an anticoagulant.
And if he has had a heart attack such person is likely to show on and
EKG (electrocardiogram) an abnormal pattern, and is given an arrhythmia drug. A
protein pump inhibitor (PPI) is added
ulcer prevention. Typical drugs
following a myocardial infarction (MI) averages $70,000 per year. Moreover,
over half of seniors age 65 to 74 are
on statins, and 40% of men 55 to 64. For
women the number is a bit lower. Pharma
is very good at marketing.
Understanding the role
of atherosclerosis in the development of
CVD is necessary for rational, evidence-based heart choices. Atherosclerosis
is caused by pathogens within the
artery walls and the immune system’s response [See LDL illustraton, top].
This response results in the formation of unstable young plaque within
the lumen of arteries which over a period of several years will become harden
(stable plaque). The unstable plaque which
causes only a slight constriction at most of the artery causes over 80% of MIs
(myocardial infarctions, heart attacks) & 85% of strokes. (Retain this essential relationship.) Thus even those without CVD
are at risk for MI and stroke because they are very likely forming some young
unstable plaque, the rate of which can vary according to a number of factors,
the most important being diet, reactive chemical, chronic infections, and
drugs.
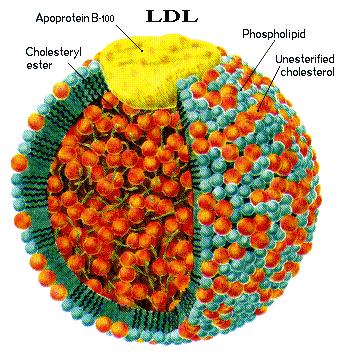
Understanding the role
of damaged LDL in the development of AS: LDL (see illustration above)
consists of chains of fatty acids with about 6 apolipoproteins molecules.
They form a ball with about
1,500 cholesterol molecules in interior of the ball and 3,000 to 6,000
triglycerides (see illustration at top of page). Fatty acids (including those
in
triglycerides) and cholesterol are not blood/water soluble. Lipoprotein with
attached acid end of the
triglyceride form LDL which is water soluble. LDL is produced in the liver for
transport of cholesterol and fatty acids to cells as needed throughout the
body. During that transport process in
the blood and when taken up by the arteries, the LDL can become damage by superoxides and by glycation[7]. More
important is the fact that LDL has on its surface antibodies which
permit it to attach to pathogens and some of the toxins they produce. This function
has been known for a hundred
years-- read Prof. Uffe Ravnskov’s book Ignore the Awkward! p 136-140.
“In the laboratory it has been shown that human LDL is able to
inactivate more than 90% of most toxic bacterial products” supra. 138. This is
but one of a number of confirmatory experiments on LDL’s immune-system function.
Multiple functions are the norm in animal
biology. Insulin for example has listed
over a dozen functions--see Wikipedia
. This function fits in neatly: the
LDL is actively transported into the
tunica media of the artery because of its immune system function. It also explains
why lymphocytes including
the scavenger macrophages are in the tunica media. Pharma’s claim simply
doesn’t make sense that
LDL would be in the tunica media in sufficient concentration in a tissue with a
low rate of metabolism and thus low requirements for cholesterol and/or
triglycerides. Certain tissues of low
activity are prone to infection, and given the autopsy evidence, the tunica
media is one of them. Given the
presents of white blood cells, it
must be in the immune function which accounts for the presence of LDL. Pharma’s
oxidation theory within the tunica
media is counter the normal function for LDL.
And why in the tunica media instead of in the plasma where there are
more reactive chemicals? Pharma makes no
mention of pathogens in the tunica media.
Rather they hold that the inflammatory response involving leucocytes is
due to injury (See Braunwald Heart Disease
5th Ed.,
1113-1115). There is no mention of
pathogens by Braunwald, though there are 100s of journal articles on pathogens
within the artery walls. An excellent
summary of the evidence is in The
Great Cholesterol Con by Anthony Colpo, at 207-215. There
are two stories one Ptolemaic, the other Copernican; one complex and
far-fetched, the other simple and within the norm of immune system
function. One ignores evidence of
pathogens, the other doesn’t.
Lack of association between
hypercholesterolemia and CVD: This association has been put forth
as proof of that A causes B. As stated
earlier being a bystander does prove causation, and that the cause is reactive
chemicals which overload the cleanup system or damage LDL by macrophages. Thus
according to pharma’s model those with
more LDL would be have a higher rate of damage.
But there is a problem with this model, since the presents of LDL is
through active transport into the tunica media, higher serum cholesterol would
entail more than needed levels of LDL in the tunica media. This is confirmed
in numerous studies of
those with high cholesterol as to the rate of atherosclerosis and the
subsequent MI (myocardial infarctions, heart attacks). Those with familial
hypercholesterolemia
(level due to a genetic defect that are at least double the level considered
high) do not have significantly more heart attacks or die significantly sooner
than those with normal level (at least in older studies before the use of
statins). One would expect a strong
association, but studies only find a minor association, at most—see Uffe at. The failure to find an association of elevated
TC with MI is thoroughly described in the books by Uffe and Colpo
supra. I go over this evidence at and also. There are numerous books in
addition to the two mentioned which expose this myth, just visit Amazon to find
them, or watch the documentaries.
Atheroma: “The atheroma (accumulation
& swelling in
an artery wall) consists of LDL [see illustration],
calcium, fibrous connective tissues, T-lymphocytes macrophages, and pathogens. While in the early
stages, based on gross appearance, have traditionally been termed fatty streaks by pathologists, they are not composed of fat cells (adipose cells), but are accumulations of
white blood cells, especially macrophages, that have taken
up damaged low-density
lipoprotein (LDL). After they
accumulate large amounts of cytoplasmic membranes (with associated high
cholesterol content) the macrophages are called foam cells. When foam cells die,
their contents are released, which attracts more macrophages. Left out of this
pharma tale is the fact that
macrophages can be damaged by the toxins produced by bacteria—see and,
possible including those which are found on the surface of LDL antigens.
Coronary artery
disease (CAD), hypertension & CVD, pharma’s version: Atherosclerosis
affects coronary arteries and thus the blood supply to the heart muscle. “Atherosclerosis
is the most common type of heart disease and cause of heart attacks. The disease is caused by plaque building up along the
inner walls of the arteries of the
heart, which narrows the arteries and restricts blood flow to the
heart. It is the leading cause of death worldwide.[1]
After decades of progression, some of the atheromatous plaques may rupture
and (along with the activation of the blood clotting system) start limiting blood flow to the heart muscle. The disease is the
most common cause of sudden death,[2] and the leading cause of death over the age
of 20 years.[3] Most
commonly,
unstable young plaque ruptures and may lead to an acute myocardial
infarction (AMI). Cholesterol
is delivered into the vessel wall by cholesterol-containing low-density
lipoprotein (LDL) particles. To attract and stimulate macrophages (a type
of white cell), the cholesterol must be released from the LDL particles and
oxidized, a key step in the ongoing inflammatory process” Wiki. “The process is worsened if there is
insufficient high-density
lipoprotein (HDL). The lipoprotein
particles [HDL] remove cholesterol from tissues and carry it back to the
liver. When the macrophages [type of
white blood cell] engulf a large amount of the oxidized cholesterol [as part of
the disposal process] they are called foam
cells because of appearance. In sufficient numbers they form the
fatty streaks of the plaques of atheroma in the innermost layer of the artery
wall. A protective fibrous cap normally
forms between the fatty deposits and the artery lining (the intima).
These capped fatty deposits (now called 'atheromas') produce enzymes
that cause the artery to enlarge over time. Atheromas within the vessel wall
are soft and fragile with little elasticity. Arteries constantly expand and
contract with each heartbeat, i.e., the pulse. In addition, the calcification
deposits between the
outer portion of the atheroma and the muscular wall, as they progress, lead to a loss of
elasticity and stiffening of the artery as a whole” Wiki. Pathogens
are not mentioned, nor is the young unstable plaque compared to a boil. Pharma
focuses on occluded vessels by mature
plaque, upon elevated TC and HT.
Hypertension thus is a trailing result not a cause of AS. The higher risk of ischemic events (MI and
ischemic strokes) that occurs with HT
is a result of a statistically higher rate of atherogenesis & thus young
plaque. [8] To lower blood pressure does not significantly
affect unstable plaque the cause of acute ischemic events. Macrophages during
their cleanup function
weaken the protein matrix and thereby increase the risk for the young plaque
will leak out of the lumen. A person with HT is more
likely to have a clot form at the point where the plug has limited the flow of
blood. HT contributes to the
clotting process; but not to atherogenesis.
HT is mere a sign of atherogenesis, which causes ischemic
events. MIs often occur
with normal blood pressure and normal TC. AS, oxidative damage
to LDL, and unstable
young plaque are not treated by Pharma’s drugs, thus they stresses TC
and HT to promote sales.
Most atherosclerotic formations are the result of infections
in the tunica media.
“Cytomegalovirus (CMV) infection is also associated with cardiovascular
diseases.[13] In time, as cells die, this leads to
extracellular calcium deposits between the muscular wall and outer portion of
the atheromatous plaques. The
accumulation of calcium leads to a loss of elasticity and stiffening of the
artery as a whole [one cause of hypertension]
“ Wiki. A number of chronic conditions are
contributors to CVD: women with rheumatoid arthritis have “double
the risk of heart attacks when compared to women without it… An infection that
starts in the gums, for example, can easily lead bacteria into the blood-stream
that may find fertile ground in a weakened arterial wall and fan the fires of
inflammation there” (Bowden 45). Thus
infection is a cause of AS. Note
how Wiki consistently fails to mention
the presence of pathogens in the artery walls—a clear sign of pharma’s
influence.
The infection vector in the causes of AS consists of a direct involvement through infection within the artery lumen, and
an indirect through chronic
infection. Among chronic infections, the
Helicobacter pylori (the cause for over 80% of ulcers) increase the risk
of MI by 75%. “A
number of acute and chronic infections including: Chlamydophila pneumoniae, lupus
erythematosus, influenza, and Porphyromonas
gingivalis [gingivitis] among others
have been linked to atherosclerosis and myocardial infarction” Wiki. “Women with rheumatoid
arthritis, a highly
inflammatory condition that primarily affects the joints, wind up having double
the risk of a heart attack…” (Bowden 45).
Within the artery lumen Cytomegalovirus, herpes virus
and several other pathogens have been found upon examination during autopsy
examinations.
The immune response of LDL is also documented: “Antibodies to
oxidized LDL (ox-LDL) and LDL-containing immune complexes (LDL-IC) have been
reported to be associated with the presence or progression of arteriosclerosis”
at. “Antibody is a large, Y-shape protein produced by plasma cells that is used by the immune system to identify and neutralize pathogens such as bacteria and viruses” Wiki. These antibodies on LDL are
further indication of their immune function.
Moreover long-term test for C-reactive protein (CPR) is a better predictor of ischemic
events in men followed long-term than that of elevated LDL. CPR
is a marker for infection[9]. Further support is found in that NSAIDs
down-regulate COX-2 prostaglandin and thereby increase acute ischemic events
through inhibition of the immune system which is found to promote the
atherogenic process--(aspirin is the only known COX2 inhibitor that doesn’t
promote AS).[10] Given the role of oxidative damage to LDL and
the inflammation response, lowering LDL can at best have only a minor
effect. The current attempts to prevent
the consequences of AS do not address
its two major causes:
damage to LDL and the subsequent immune response. A review of the first 50 citation
for
“infection + atherosclerosis” found not one article published after 2003 on
infection as a cause for atherosclerosis but for 3 on HIV. A promising area
of research is not being
funded because of pharma and their friends.
Since pharma is driven to maximize
profits, thus treating disease not preventing them. They treat signs as though
they are diseases
and anything else that will up profits.
So how does pharma handle the evidence of the immune function of LDL?
The
oxidized LDL myth as cause of atherosclerosis: Oxidized means a chemical reaction involving
the sharing or transfer of electron. Thus
a toxin, virus, or bacteria bonding (attaching) counts as oxidized. For pharma
the cause of oxidized LDL caused
by reactive chemical byproducts from
metabolism and this occurs in the tunica media, where the plaque forms. Then
lymphocytes enter the tunica media,
spot the oxidized LDL and signal for the specialized macrophages which then
enter the tunica media, and devour the oxidized LDL. Upon ingesting too many
of these damaged LDL,
the macrophages are converted to foam cells (swollen macrophages)
which then undergo apoptosis (cell death).
The debris from the apoptosis which consists mostly of triglycerides and
cholesterol from the ingested LDL, if sufficient, will form plaque, the foundation
for the development of AS.[11] Nice
story, but unlikely. Unlikely
because 1) in a biologically inactive area (unless there is an infection and
healing process), the tunica media, there is not a need for LDL. LDL occurs
in metabolically active areas
where its contents of fats and cholesterol are
used in cell building. 2) This area
of low activity will not produce very many reactive byproducts of metabolism to
attach to LDL and oxidize them. Should
not this plaque forming process according to pharma’s theory be most prevalent
in areas of high metabolism? 3) It has
not been shown that leucocytes start an inflammatory process because of a few
oxidized LDL. However leucocytes primary
function is to respond to toxins, foreign matter, and pathogens. LDL is a protein
rap around cholesterol and
fat molecules that travels to tissues as needed. 5) Polyunsaturated fats have
been
demonstrated to be subject to a process of oxidation by reactive chemicals,
most of which come from products of metabolism; however, these oxidize fats do
not cause an immune system response.
This is more evidence that oxidation is not the cause of the
inflammatory response. Note: the
problem with these rancid fats is that
the body lacks enzymes for their disposal.
Their accumulation, like transfats, contributes to the atherogenic
process. 6) It has not been shown that
the macrophages would ingest oxidized LDL—unless they had on their surface
antibodies with toxins or pathogens attached thereto. 7) Pharma then hypothesizes
that our body
makes antibodies which recognized oxidized LDL attach to it, and thereby causes
the immune response. However it is the
LDL with immune complex that have occupied sites that are shown to be subject
to digestion by macrophages, at. “These results
indicate that the binding of lipoprotein immune
complexes to Fc receptors on monocytic cells activates a series of responses
that could accelerate the initiation or progression of atherosclerosis” at. Pharma’s story of AS being caused by reactive chemical
attached to LDL is far-fetched: it
creates new process occurring in low metabolic area; and it ignores the volumes
of articles on pathogens in atheroma.
Big pharma has frames the discussion of AS in a way that has researchers
looking under the wrong bush.
Lowering
LDL is irrelevant: Since the presence
of LD in the tunica media involves active
transport, lowering the serum level of LDL doesn’t impact the number of LDL
actively transported by the epithelial cells.
Corollary having a high level of LDL doesn’t increase its presence in
the tunica media, this explains the lack of association between level of cholesterol,
LDL and coronary artery disease, and why drugs which lower them aren’t worth
their side effects—see cholesterol
myth.
The
evidence that LDL has an immune system function: “In the laboratory it has been shown that human
LDL inactivates more than 90% of most toxic bacterial products” Uffe supra at
138. Lipoproteins in experiments inhibit
endotoxins.[12] “When Kenneth Feingold and his co-workers at
the University of California in San Francisco reduced blood cholesterol in
rates [thus also LDL] and gave them an injection of bacterial toxin, most of
them died quickly, but if they injected purified human LDL beforehand they
survived” Uffe Supra 138. A similar mechanism in which lipoproteins
neutralize E. coli, N. meningitides , and complete Gram-negative bacteria-- full. “Thus, lipoproteins, in addition to playing a
role in lipid transport, may have protective functions” Feingold 1995. The LDL is homocysteinylated and oxidized
lipoprotein aggregates
complexed with microbial remnants and LDL auto-antibodies
are found in the Vasa Vasorum
(blood vessels that nourish the tissue with in larger arteries).[13] There is a large body of experimental evidence
to confirm the immune function of LDL.
This function along with transporting the materials for building cell
walls (cholesterol and triglycerides) explains why they are actively
transported through the epithelial lining of artery walls; they are need for this
function. An intervention which interfered
with this healing function is dangerous.
What
really causes atherosclerosis:
Pathogens living in the tunica media cause an immune response from both
their physical presence as foreign matter and biotoxins which they release that
cause cellular. In response to their
presence and the biotoxins the endothelial cells then actively transport LDL
with antibodies on their surface for to attack the pathogens and absorb their
toxin--see. The endothelia cell also signal for
leucocytes to fight the infection. The
leucocytes then signal for macrophages to assist. The macrophages engulf pathogens,
toxins, and
the toxin laden LDL.[14] An overload of toxins, pathogens, and toxin
laden LDL results in apoptosis (program cell death) of the macrophage with the
release of its contents. This infection
process if sufficiently vigorous will result in the formation of plaque, in
much the same way a boil forms under the skin because of an immune response to
bacterial activities. In fact Uffe
refers to this process as being similar to that of the formation of a
boil. “… the vulnerable [young] plaque
is a pustule, a small boil” Uffe supra 138.
The results of NOT accepting
pharma’s model for AS is tragic:
doctors are prescribing and patients take drugs which do not affect the
progression of atherosclerosis, and they undergo invasive procedures which do
not reduce risk of acute events and deaths from CVD, while effective alternative
are criticized based upon pharma’s
tobacco science. Moreover researchers
are looking under the wrong bush. A
review of the first 50 citation for “infection + atherosclerosis” I found not
one article published after 2003 on infection as a cause for atherosclerosis—I
excluded the 3 which were on HIV,
because HIV is known to compromise the immune system. A promising area of research
is not being
funded because of big pharma.
Unstable
plaque, the wild card: unstable plaque
is fresh,
young plaque that forms within the lumen of an artery. It doesn’t show up in an angiograms,
because occlusion is under 20%. Testing for
infection is only moderately associated with the process. The
measure of C-reactive protein is only weakly associated with plaque formation,
since such infections are often minor and temporary. Infections in the tunica
media are nearly always without symptoms.
Macrophages in their cleanup healing role for young plaque
“secrete cytokines and protease that weaken the fibrous cap, causing it to
erode or rupture. The newly exposed sub-endothelium
and pro-coagulant factor precipitate platelet aggregation and local thrombus
formation, sometimes leading to infarction [MI]” AHA,
2013. The
best way to reduce this risk for the formation of unstable, young plaque is to
improve immune functions and overall health through a healthful diet, one that
is similar to those of our poorer ancestors two centuries ago. The effects of
fatty liver, IR, fructose, refined carbs, unhealthful
polyunsaturated and transfats, and carbon monoxide from cigarettes have
cumulatively brought about atherosclerosis with its consequences and a host of
other conditions.
Some positive choices: Everyone by the age of 40 has some young
plaque, especially males. Women are protected by estradiol, this is why contra-pharma,
post-menopausal women should take natural HRT for cardiovascular
protection.[15] Past attempts—1950s to 1980s--to find an
estrogen analog for men have failed.[16] The sex hormones, in their androgen effect,
promote healing. Estrogen, for example,
has been shown “to promote the resorption of extras-cellular lipids [constituents
of plaque] and reversal of endothelial dysfunction” AHA. In addition it protects LDL from oxidative
damage (see myth 12 above). Testosterone also has been shown
to be protective: those elderly men whose
level is the top 20% have a very significantly lower incidence of death from CVD.
However
the most important risk reduction comes from a healthful diet and maintaining a
healthy liver (see above myths 7 through 17). There is a library of technical
materials on
diet at the rh
website section including links to the best of documentaries and academic
lectures on the topics discussed.
Remember that metabolic dysfunction caused by the Western diet is 80%
reason for the difference is rates of CVD,
cancer, Alzheimer’s disease, arthritis, osteoporosis, and a host of other
conditions between us and those who eat a paleo-diet, or the peasant’s diet of
Orientals and Europeans two centuries ago.
[1]
Klotz O. Manning, J. of Pathol Bacteriol 1911:16:211-20. “There is every
indication that the production of tissue in the intima
is the result of a direct irritation of that tissue by the presence of
infection or toxins.”
[2]
“Monocytes are a type of white
blood
cell. They
are the largest of all leucocytes. They are part of the innate
immune system of vertebrates including all mammals (humans included), birds, reptiles, and fish. They are amoeboid in shape, having clear cytoplasm. Monocytes have bean-shaped nuclei and constitute 2-10% of all
leucocytes in the human body. Monocytes play multiple roles in immune function.
Such roles include: (1) replenishing resident macrophages under normal states, and (2) in response to inflammation signals, monocytes can move quickly (approx. 8–12
hours) to sites of infection in the tissues and divide/differentiate into
macrophages and dendritic cells to elicit an immune response. Half of them are
stored in the spleen” Wiki.
[3] “Macrophages are cells produced by the differentiation of monocytes in tissues.
Macrophages
function in both non-specific
defense (innate
immunity) as well as help
initiate specific defense mechanisms (adaptive
immunity) of vertebrate
animals. Macrophages have the unique ability to metabolize one amino acid,
arginine, to either a "killer" molecule (Nitric Oxide) or a
"repair" molecule (Ornithine). Macrophages predominantly expressing
the killer or repair phenotype are now mainly called M1 or M2 macrophages
because these 2 types of macrophages also stimulate T cell responses that
further activate the killer macrophages or T cell phenotype (Th1), or stimulate
antibody production (Th2).[4] Their role is to phagocytose, or engulf and then digest, cellular debris and pathogens, either as stationary or as mobile cells. They
also stimulate lymphocytes and other immune cells to respond to pathogens.
They are specialized phagocytic cells that attack foreign substances,
infectious microbes, and cancer cells through destruction and
ingestion. They are present in all living tissues, and have a function in regeneration. Macrophages are highly specialized in removal
of dying or dead cells and cellular debris. Macrophages are the predominant
cells involved in creating the progressive plaque lesions of atherosclerosis” Wiki. It is the role of
dealing with oxidative damaged LDL that causes atherosclerosis.
[4]
Smith & Pickney in The Cholesterol Conspiracy: “Drugs were
used to lower blood cholesterol
level in twelve trials…. Of the eight that met this standard (randomized and
double blind), total deaths in six trials were the same or greater in the
treatment group than in the control group.
For the remaining 4 trials there were no difference between the trial
group and the control group;” taken from Bowden and Sinatra, The
Great Cholesterol Myth, p. 98.
For trials using drugs and diet were the same for the endpoint
death. But pharma controls the
production of information, and these results are ignored.
[5]
When atherogenesis
stops the body will undergo a healing process that will reduce occlusion of
arteries and improve through revascularization of the blood flow—a process that
takes years for a significant improvement.
For example untreated angina pain will diminish gradually and physical
endurance will increase following a MI. Pharma claims that statins remove
plaque, the truth of which is doubted because of lack of in vitro evidence,
bias in their marketing studies, and the lack of a suitable comparison cohort
in carotid artery sonogram studies. Moreover,
it isn’t hard plaque, what is measured, but the soft plaque that causes MIs.
Even if statins slow the process of atherogenesis and the bodily processes
remove account for the reduction in plaque, what its affect on soft plaque? Moreover,
aspirin and Q10 perform better. The topic is complex, see item #4, 6 & 2
under 10 negative effects in Statins.
[6] Lipitor is all time leading drug
world-wide based on dollar sales. For
statins a 2008 study found that 50% of men and 36%
of women age 65 to 74 had taken a statin in
the last 30 days.
[7] Other sources of reactive oxygen
include carbon monoxide from incomplete combustion; two main sources are
cigarettes and car exhaust. Sulfur
trioxide from combustion is another airborne source. Various metabolic reactions
also produce
reactive oxygen.
[8] It has been noted that with HT there is a response in the
endothelium cells that accelerates the thickening of the artery wall in
response to the increased blood pressure (see). Thicker
walls means that the plaque is less
likely to leak (cause MI). The
increase in blood pressure is initiated
by AS in over 90% of cases. Genetic,
drugs, and prolong emotional stress
which produces an excess of certain neurotransmitters can increase blood
pressure.
[9] Downplaying infective cause
entails not promoting testing long-term CRP.
Since CRP
is elevated during an infection, a short-term elevation is misleading, because AS
develops over decades. Women under the age of 55 are protected by
estrogen, thus including them in a study is also misleading are doing
short-term CRP testing are two ways
for pharma to tweak results as desired.
[10] PTGS2 (COX-2) is unexpressed
under normal conditions in most cells, but elevated levels are found during
inflammation. Since PTGS2 (COX- is generally expressed
only in cells where prostaglandins are upregulated (e.g., during
inflammation), drug-candidates that selectively inhibit PTGS2 (COX-2) were suspected
to show fewer side-effects [4] but proved to substantially increase risk
for cardiovascular events such as heart attack and stroke. Studies with human pharmacology and genetics, genetically manipulated rodents, and other animal models and randomized trials
indicate that this is due to suppression of PTGS2 (COX-2)-dependent
cardio-protective prostaglandins, prostacyclin in particular” Wiki. VIOXX and Celebrex
where shown to with long-term usage to at least triple in the elderly the rate
of MI, and deaths therefrom—see.
[12]
LPS is lipopolysaccharides, which is another name for endotoxins. A toxin is a
poisonous substance, and LPS are within bacteria found on the
outer membrane of gram-negative bacteria. “The LPS-inactivating capacity of
serum was shown to be a function of the lipoproteins. Other serum components,
such as naturally occurring anti-LPS immunoglobulin G, complement, or nutritive
lipids, had no significant influence in our system. Our experiments suggest
that serum
lipoproteins control endotoxin-induced monocyte activation and monokine release”
at. Endotoxins are
lipopolysaccharides from within bacteria found on the outer membrane of
gram-negative bacteria. Monokines
are cytokines are small proteins that are important in cell signaling (but not
hormones). They are released by many
different kinds of cells, including leucocytes, which is their source in the
experiment above.
[13] “Little
attention has been paid to the function of lipoproteins as part of a
nonspecific immune defense system that binds and inactivates microbes and their
toxins effectively by complex formation. Because of high extra-capillary tissue
pressure, aggregates of such complexes may be trapped in vasa vasorum of the major arteries” short by Ravnskov
and McCully, full.
[14]
These results indicate that the binding of
lipoprotein immune complexes to Fc receptors on monocytic cells activates a
series of responses that could accelerate the initiation or progression of
atherosclerosis”
at.
[15]
Prempro, a horse estrogen from mare’s urine along with medroxyprogesterone—the
worst of the progestins—to produce the poor results in a major clinical trial,
the Women’s Health Initiative. The
results of this trial were used to attack the then popular use of HRT by
menopausal and post-menopausal women—for details.
[16] In the 50s through 80s extensive
research was done looking estrogen type protection from CVD for men. None were
marketed because these analogues blocked testosterone, and thus caused ED and
loss of strength. Today prevention
doesn’t fit pharma’s business model thus costly clinical trials are not funded
and there is now very little basic laboratory research.
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^
Appendix
on why the cholesterol myth persists
If you hear 20 times “Iraq has weapons of mass
destruction” from our President and his cabinet, and it is patriotically
carried by the corporate media, and just 1 time you hear from a marginalized
critic who is subsequently rebutted by an “authority”; the vast majority of
people will believe the President; the same with bad cholesterol as the cause
of CVD. But the early clinical
trials were all negative. “In effect,
the clinical trial data overwhelmingly demonstrated no benefits of
cholesterol-lowering for either coronary heart disease deaths, nonfatal coronary
heart disease events, or all causes of deaths.”3 The cholesterol
myth gains momentum through
acceptance by patient’s peers and family doctors. The logic is attractive: those with cholesterol above 240 have about
50% of myocardial infarctions (MI, heart attacks). But A
occurring with B doesn’t mean
that A causes B. If
so then old age causes heart attacks,
because 95% of them occur past the age of 60.
Bad logic based on high total cholesterol (TC) with
the false vision that it clogs arterial like mineral a pipe and drug sales
easy. Yes, cholesterol is in artery
plaque, but it does not cause plaque.
Oxidative damage and glycation to LDL which transports cholesterol
starts the chain leading to CVD; cholesterol and triglycerides are there
as a bystander. So when 2 top scientists, Edward Pinckney and
Russell Smith, wrote “The Cholesterol
Conspiracy” most people dismissed it without reading. People remember
the Marketing Science that
high TC causes CVD. First pharma sells the condition,
hypercholesterolemia as the cause of CVD, than pharma sells the drugs to
lower cholesterol, plus drugs to ameliorate the effects of CVD. And just
like the war in Iraq, these drugs
aren’t winning the war on cholesterol and its off-spring acute ischemic
events. Given the increase in obesity
and CVD, we must question not just the role of cholesterol but all
accepted truths. There is a fundamental
conflict between profits and the public’s well-being. The
health industry has gained de facto
control of the regulatory processes. The
cholesterol myth is good for marketing their patented drugs.
The
short answer is the 800 lb. gorilla[1] has a firm grasp upon the generation & dissemination
of information. As the author
of "The
Guide to the 4,000 Useful, Useless or Dangerous Medicines"
(published in French) Dr. Philippe Even told The Guardian in Sept. 2012:
“The
pharmaceutical industry is the most lucrative, the most cynical and the least
ethical of all the industries. It is like an octopus with tentacles that has
infiltrated all the decision-making bodies:
world health organizations, government agencies, parliaments, high
administrations in health and hospitals and the medical profession." Pharma
is run
by its marketing department. For example, published journal trials average
32% positive bias. Pharma
funds and thus runs directly or indirectly clinical trials[2],
from which they arm their thought
leaders with marketing science to “educate” physicians in the mandated
continuing education classes on drugs.
Pharma with the same Marketing Science and their opinion leaders spin the contents in
medical textbooks, the clinical guidelines, Wikipedia’s articles, and the media’s
health articles. All this is carefully
scripted for to create the illusion of independence and balanced. Industry ghost
writing is common. As Dr. Ben Goldacre states in Bad Pharma: “We
no longer have evidence based medicine; we now have expert-based medicine with
pharma providing the experts. A perverse
system produces perverse results.” So
what follows in these 8 sections is the scientific
base of information on diet, CVD, obesity,
and treatments
Pharma’s drugs for the
cholesterol myth: oxidation
and glycation of LDL & the subsequent immune response is the cause of
atherogenesis; this entails a minor role of high TC and hypertension (HT)
in atherogenesis and CVD. Though
well supported by journal articles,
this is not taught by pharma thought
leaders, nor found in pharma friendly corporate media. This is because there are 4 classes of drugs that pharma hawks to treat cardiovascular
disease based upon a claim that they dramatically reduce the devastating risks associated
with cardiovascular disease (CVD).
The 4 classes are Statins to lower total
cholesterol (TC), antihypertensive
drugs to lower blood
pressure, anticoagulant
drugs to prevent
the blood clots that cause acute ischemic events, and arrhythmic
drugs to prevent
irregular heart beat that cause sudden deaths—the links are to
their critical reviews. These drug
families have been critical analyzed and found to be wanting; viz. their
benefits are not worth their side effects (and there are better treatments). Statins are supposed
to
prevent and slow the progression of CVD by lowering TC, its
putative primary cause. Hypertension (HT),
the putative second major cause of CVD, is treated with antihypertensive
drugs; but atherosclerosis (AS) is the primary cause of CVD; not high
TC & HT—signs of a process does not mean causes. HT is a
result of constricted and stiff
arteries. To assure an adequate blood
supply the heart pumps harder. Atherogenesis
occurs only when the rate of damage to LDL overwhelms the cleanup process. Lowering
TC and blood pressure does
not affect the process. I strongly
recommend that you visit the page on documentaries available for free on
YouTube, and watch the ones under the CVD section.
[1]
A phrase used by Marcia Angell to describe Big
Pharma with its billions and lobbyists.
Her book The Truth About Drug Companies
describes chapter by
chapter the gorilla’s grip—link to a chapter. Of all books, I recommend hers first.
[2] A contract with the researchers establishes
pharma’s rights as owner of the clinical trail.
This include withholding negative results, side effects, switching
end-points, etc. Moreover the raw data,
which is essential for a journal peer review panel, is always withheld, thus peer
review is a facade. The 32% average positive bias referred to
above was uncovered by researchers who obtained under the federal Freedom of
Information Act (FOIA) the raw data pharma had submitted to the FDA. Those trials
were subsequently
published. A pile of published evidence
supports that bias (tobacco science) is the norm.
|